A high-yield, consultant-level guide to burns in the Emergency Department, aligned with Final FRCEM SBA exam expectations. Covers burn types, ABCDE assessment, airway and inhalation injury, fluid resuscitation, escharotomy, referral criteria, and common exam pitfalls—with direct links to RCEM and UK national guidance.
Burn injuries are high-impact, high-yield topics in the Final FRCEM examination. They test not only factual knowledge but situational judgement, early recognition of deterioration, and prioritisation using an ABCDE framework—all core consultant competencies.
In the UK, approximately 130,000 patients attend Emergency Departments annually with burn injuries, with around 8% requiring admission. Despite representing a minority of trauma presentations, burns carry disproportionate morbidity and mortality, particularly in children, older adults, and vulnerable populations.
For Final SBA candidates, burns questions frequently integrate:
A burn is a traumatic injury to skin or other organic tissue, caused primarily by thermal or other acute energy exposure.
🔥 Thermal Burns (Most Common)
Exam tip:
Scalds dominate paediatric cases, while flame burns are more common in adults.
🧪 Chemical Burns
Key SBA principle:
Alkali burns (e.g. cement) require immediate and prolonged irrigation and often present deceptively mild initially.
⚡ Electrical Burns
Always perform an ECG, even in low-voltage domestic injuries, due to arrhythmia risk from alternating current.
❄️ Cold Injury (Frostbite)
☢️ Radiation Burns
Final SBA red flag:
Always actively exclude non-accidental injury in children and vulnerable adults.

Exam insight:
Poor resuscitation converts the zone of stasis into necrosis.
Mechanisms of compromise
High-risk features
Management
Common SBA pitfall:
Failure to predict progressive airway compromise.
Threats
Key actions
Learning point:
Cyanide poisoning is common in enclosed-space fires—consider early hydroxocobalamin in refractory hypoxia.
Burns >20% TBSA can cause burn shock, but isolated burns rarely cause immediate hypotension—always search for alternative causes.
Assessment
Investigations
Indications
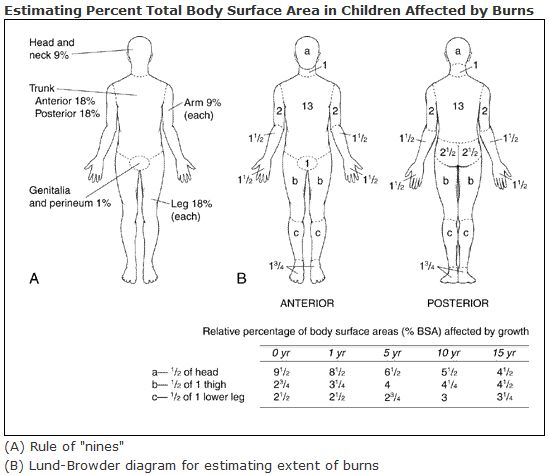
- Adults: >20% TBSA
- Children: >10% TBSA
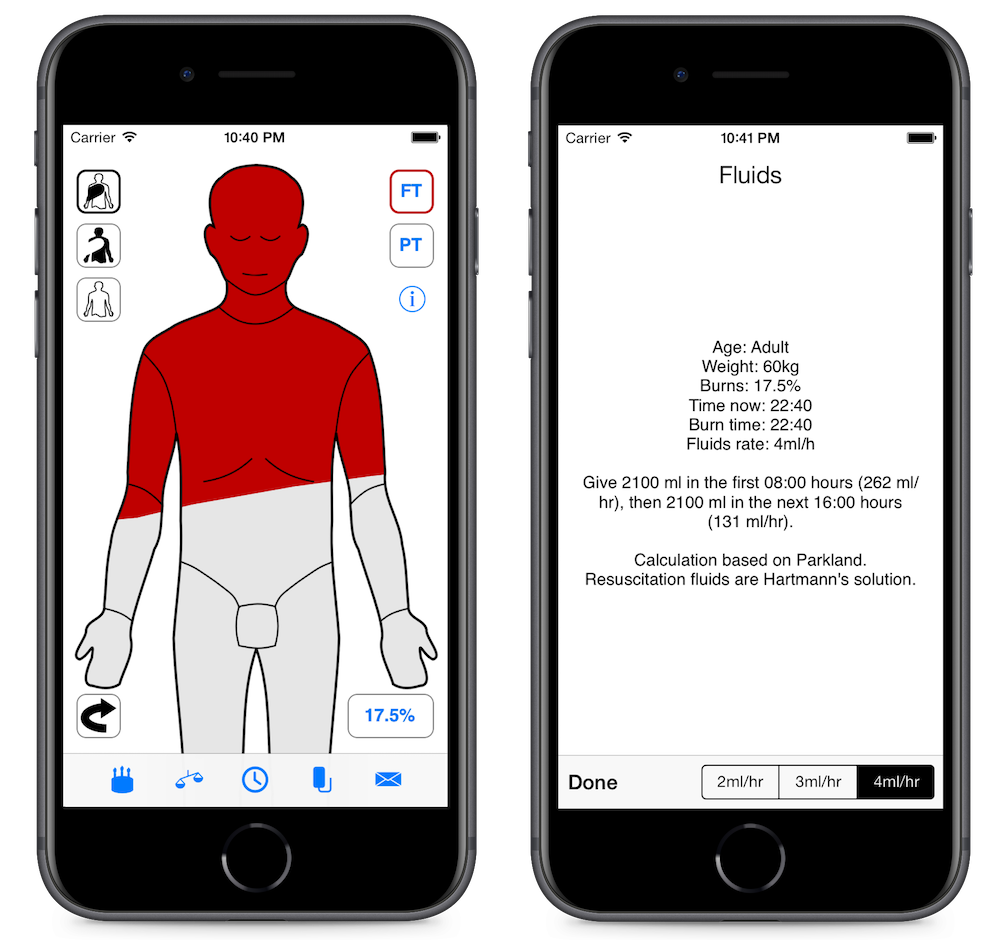
Formula
2–4 ml × weight (kg) × %TBSA
Urine output targets
Consultant-level tip:
Coordinate exposure, assessment, and photography once, with the whole team present, to reduce heat loss.

Exam rule:
Epidermal (erythematous) burns are NOT included in TBSA calculations.
For ED decision-making:
Only two distinctions matter:
Asymptomatic patient + normal ECG → no prolonged cardiac monitoring required.


Indications
Principles
Final SBA pearl:
Escharotomy is a time-critical emergency, not a theatre-only procedure.